HERBAL
MEDICINAL
PLANT

DEVIL’S CLAW
Harpagophytum procumbens (Burch.) DC ex. Meisn. (Pedaliaceae) ++
BY
RETTODWIKART THENU
DEVIL’S
CLAW
(dev’uhlz
claw)
Harpagophytum procumbens (Burch.) DC ex. Meisn. (Pedaliaceae) ++
SUMMARY AND PHARMACEUTICAL COMMENT
The
botanical name Harpagophytum means ‘hook plant’ in Greek, after the
hook-covered fruits of the plant. Devil’s claw is native to southern Africa and
has been used traditionally as a bitter tonic for digestive disturbances,
febrile illnesses and allergic reactions, and to relieve pain (Mills
& Bone 2000). It has been used in Europe for the treatment of rheumatic
conditions for over 50 years, and was first cited in the literature by Zorn at
the University of Jena, Germany, who described his observations on the
antiphlogistic and anti-arthritic effects after administration of oral aqueous
extracts prepared from the secondary roots of H. procumbens in patients
suffering from arthritides (Chrubasik et al 2006).
The chemistry of devil’s claw has been well documented. The iridoid
constituents are thought to be responsible for the reputed anti-inflammatory
activity of devil’s claw, although it is not known precisely which of these are
the most important for pharmacological activity, and the importance of other compounds.
There is conflicting evidence from in vitro, animal and human studies regarding the anti-inflammatory activity
of devil’s claw and possible mechanisms of action.
Several randomised trials using devil’s claw extracts standardised
on harpagoside content have reported superiority over placebo for some aspects
of low back pain and rheumatic complaints. However, some studies used
nonstandard outcome measures and carried out several post-hoc analyses. Further
studies have used recognised, predefined outcome measures to establish the
therapeutic value of standardised devil’s claw extracts in patients with
arthritic and rheumatic conditions.
On the basis of randomised controlled trials involving patients
with arthritic and rheumatic disorders, devil’s claw extracts appear to have a
favourable short-term adverse effect profile when taken in recommended doses.
Mild, transient gastrointestinal effects, such as diarrhoea and flatulence, may
occur. Chronic toxicity studies and clinical experience with prolonged use are
lacking, so the effects of long-term use are not known. On this basis, and in
view of the possible cardioactivity of devil’s claw, devil’s claw should not be
used for long periods of time at doses higher than recommended.
Further studies involving large numbers of patients are required.
TRADE NAMES
Devil's
Claw (available from a number of manufacturers),
Devil's
Claw Secondary Root, Devil's Claw Root Tuber
OTHER COMMON NAMES
Grapple
Plant, Wood Spider
DESCRIPTION
MEDICINAL PARTS: The medicinal
parts are the dried tubular secondary roots and the thick lateral tubers.
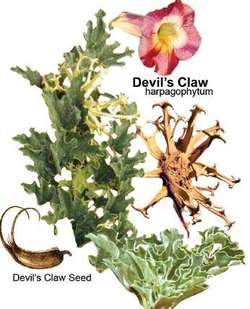
FLOWER AND FRUIT: The flowers grow
on short pedicles in the leaf axils and are solitary, large and foxglove-like.
The petals are pale-pink to crimson. The seed capsules are bivalvular, compressed
at the sides and ovate. The capsules are 7 to 20 cm long, 6 cm in diameter, and
very woody with longitudinally striped rind. They have a double row of elastic,
armL ike, branched appendages with an anchor-like hook. The capsules contain
about 50 dark oblong seeds with a rough surface.
LEAVES, STEM AND ROOT: The plant is
perennial and leafy. It has a branched root system and branched, prostrate
shoots 1 to 1.5 m long. The leaves are petiolate and lobed, and may be opposite
or alternate. The aerial parts of the plant die back in the dry season. The
tuber (storage) roots are formed from the main and lateral roots. The main
roots have obtuse, quadrangular, upright collar-like sections, 10 to 20 cm long
and 30 to 60 cm thick, which are covered in a fissured cork layer. The nodes of
the lateral roots are up to 60 mm thick and 20 cm long, and are light-brown to
red-brown on the outside. The roots extend out to an area of about 150 cm around
the plant and grow down to a depth of 30 to 60 cm.
CHARACTERISTICS: The dried,
pulverized secondary tubers and roots are yellowish-gray to bright pink and
horn-like in their hardness. They have a bitter taste.
HABITAT: The plant
originated in South Africa and Namibia, and has spread throughout the Savannas
and the Kalahari.
PRODUCTION: Devil's Claw root
consists of the dried lateral roots and secondary tubers of Harpagophytum
procumbens. The lateral roots are cut into slices or pieces, or pulverized immediately
after digging because they harden and become very difficult to cut once dry.
SPECIES (FAMILY)
Harpagophytum procumbens (Burch.) DC ex. Meisn.
(Pedaliaceae) ++
SYNONYM(S)
Uncaria procumbens Burch.
Harpagophytum, Harpagophytum burchelii Decne, Grapple Plant,
Wood Spider
ORIGIN
Devil’s claw grows wild in
southwest Africa.
PHARMACOPODIAL AND OTHER MONOGRAPHS
BHC 1992(G6)
BHMA 2003(G66)
BHP 1996(G9)
BP 2007(G84)
Complete German Commission E(G3)
ESCOP 2003(G76)
Martindale 35th edition(G85)
Ph Eur 2007(G81)
LEGAL CATEGORY (LICENSED PRODUCTS)
Devil's claw is not included in the GSL.(G37)
CONSTITUENTS
See
also General Reference G2.
Carbohydrates
Fructose, galactose, glucose and myo-inositol (monosaccharides), raffinose,
stachyose (46%) and sucrose (oligosaccharides).(1)
Diterpenes
(þ)-8,11,13-totaratriene-12,13-diol and (þ)-8,11,13- abietatrien-12-ol.(2)
Iridoids
Harpagoside (1–3%), harpagide, 8-p-coumaroylharpagide, 8-feruloylharpagide,
8-cinnamylmyoporoside, 60-O-p-coumaroylharpagide, 60-p-coumaroylprocumbide, and
pagoside.(3–5) p-Coumaroyl esters occur as E and Z isomers.(5)
Phenylpropanoids
Acteoside and isoacteoside, 6-O-acetylacteoside,( 4–6)
2,6-O-diacetylacteoside.(7)
Other Constituents Amino acids, flavonoids
(e.g. kaempferol, luteolin), triterpenoids, sterols.(4, G75)
Other Plant Parts The flower, stem and ripe fruit are reported to be devoid of
harpagoside; the leaf contains traces of iridoids.(8)
Quality Of Plant Material and
Commercial Products
According to the British and European Pharmacopoeias, devil's claw
root consists of the cut and dried tuberous secondary roots of H. procumbens DC. It contains not less
than 1.2% of harpagoside, calculated with reference to the dried drug.(G81,
G84) As with other herbal medicinal products, there is variation in the qualitative
and quantitative composition of commercial devil's claw root preparations.
Some commercial extracts of devil's claw root may have been prepared
not only from the roots of H. procumbens, but also from the roots of H.
zeyheri, which are similar macroscopically.(9) However, the two species differ
in the concentration of the constituents harpagoside and 8-p-coumaroylharpagide.
On this basis it has been stated that the species can be distinguished chemically
by determining the ratio harpagoside : 8-p-coumaroylharpagide.
The ratio is stated to be near one for H. zeyheri and between 20
and 38 for H. procumbens which has a
low 8-pcoumaroylharpagide content.(9) While this ratio may be sufficient for
chemotaxonomic differentiation, it may not be adequate for quality control.(10)
Other studies have demonstrated that the harpagoside content of
several powdered dry extracts of devil's claw from different manufacturers
varies, and that each extract has a unique profile of other constituents.(11)
The harpagoside content of commercial extracts of H. procumbens has been reported to range from 0.8– 2.3%.(12)
COMPOUNDS
Liridoide
monoterpenes: including
harpagoside (extremely bitter), harpagide, procumbide
Phenylethanol
derivatives: including
acteoside (verbascoside); isoacteoside
Oligosaccharides:
stachyose
Harpagoquinones (traces)
CHEMICAL COMPONENTS
The major active constituent is considered to be the bitter iridoid
glucoside, harpagoside, which should constitute not less than 1.2% of the dried
herb. Other iridoid glycosides include harpagide, procumbide, 8-O-(p-coumaroyl)-harpagide
and verbascoside. About 50% of the herb consists of sugars. There are also
triterpenes, phytosterols, plant phenolic acids, flavonol glycosides and
phenolic glycosides. Harpagophytum zeyheri, which has a lower level of
active compounds, may be partially substituted for H. procumbens in some
commercial preparations (Stewart & Cole 2005).
The extraction solvent (e.g. water, ethanol) has a major impact on
the active principle of the products (Chrubasik 2004a).
When administering H. procumbens extract topically it was found that
higher penetration of all compounds occurred from an ethanol/water preparation (Abdelouahab
& Heard 2008b).
USES
USES
Devil’s claw is used to increase the appetite and to
treat joint pain and infl ammation, arthritis, allergies, headache, heartburn,
dysmenorrhea, gastrointestinal upset, malaria, gout, and nicotine poisoning.
FOOD USE
Devil's
claw is not used in foods.
HERBAL USE
Devil's
claw is stated to possess anti-inflammatory, antirheumatic, analgesic, sedative
and diuretic properties. Traditionally, it has been used as a stomachic and a
bitter tonic, and for arthritis, gout, myalgia, fibrositis, lumbago,
pleurodynia and rheumatic disease.(G2, G6–G8,G32, G64) Modern use of devil's
claw is focused on its use in the treatment of rheumatic and arthritic
conditions, and low back pain.
CLINICAL USE
Arthritis
Overall, evidence from clinical trials suggests that devil’s claw
is effective in the treatment of arthritis. An observational study of 6 months’
use of 3–9 g/day of an aqueous extract of devil’s claw root reported significant
benefit in 42–85% of the 630 people suffering from various arthritic complaints
(Bone & Walker 1997). In a 12-week uncontrolled
multicentre study of 75 patients with arthrosis of the hip or knee, a strong
reduction in pain and the symptoms of osteoarthritis were observed in patients taking
2400 mg of devil’s claw extract daily, corresponding to 50 mg harpagoside
(Wegener & Lupke 2003). Similar results were reported in a 2-month observational
study of 227 people with osteoarthritic knee and hip pain and non-specific low
back pain (Chrubasik et al 2002) and a double-blind study
of 89 subjects with rheumatic complaints using powdered devil’s claw root (2 g/day)
for 2 months, which also provided significant pain relief, whereas another
double-blind study of 100 people reported benefit after 1 month (Bone
& Walker 1997).
A case report suggests that devil’s claw relieved strong joint
pain in a patient with Crohn’s disease (Kaszkin et al 2004b). A single group
open study of 8 weeks duration involving 259 patients showed statistically significant
improvements in patient assessment of global pain, stiffness and function, and
significant reductions in mean pain scores for hand, wrist, elbow, shoulder,
hip, knee and back pain. Moreover, quality of life scores significantly
increased and 60% of patients either reduced or stopped concomitant pain
medication (Warnock et al 2007).
Comparisons with standard treatment have also been investigated. In
2000, encouraging results of a randomised double-blind study comparing the effects
of treatment with devil’s claw 2610 mg/day with diacerhein 100 mg/day were
published (Leblan et al 2000). The study involved 122 people with osteoarthritis of the hip
and/or knee and was conducted over 4 months. It found that both treatment groups
showed similar considerable improvements in symptoms of osteoarthritis;
however, those receiving devil’s claw required fewer rescue analgesics. One
double-blind, randomised, multicentre clinical study of 122 patients with
osteoarthritis of the knee and hip found that treatment with Harpadol (6
capsules/day, each containing 435 mg of cryoground powder of H. procumbens)
given over 4 months was as effective as diacerhein (an analgesic) 100 mg/day (Chantre
et al 2000). However, at the end of the study, patients taking Harpadol were
using significantly fewer NSAIDs and had a significantly lower frequency of
adverse events. In a 6-week study of only 13 subjects, similar benefits for
devil’s claw and indomethacin were reported (Newall et al 1996). A preliminary
study comparing the proprietary extract Doloteffin with the COX-2 inhibitor
rofecoxib reported a benefit with the herbal treatment but suggested that
larger studies are still required (Chrubasik et al 2003b). Previously
reviews have concluded that there is moderate evidence of the effectiveness of H.
procumbens in the treatment of osteoarthritis of the spine, hip and knee; however it is suggested, as with many herbal
medicines, that evidence of effectiveness is not transferable from product to
product and that the evidence is more robust for
products that contain at least 50 mg of harpagoside in the
daily dosage (Chrubasik et al 2003a, Gagnier et al
2004, Long et al 2001).
Recently two reviews have concluded that ‘data from higher quality
studies suggest that Devil’s claw appeared effective in the reduction of the
main clinical symptom of pain’ (Brien et al 2006) and that the evidence of effectiveness was ‘strong’ for at least
50 mg of harpagoside as the daily dose (Chrubasik JE et al 2007). Nevertheless,
2 other recent reviews concluded that there was only ‘limited evidence’ (Ameye & Chee 2006) and
‘insufficient reliable evidence’ regarding the long term effectiveness of devil’s
claw (Gregory et al 2008).
The herb is Commission E approved as supportive therapy for
degenerative musculoskeletal disorders (Blumenthal
et al 2000) and ESCOP approved for painful
osteoarthritis (ESCOP 2003).
Back
pain
Several double-blind studies have reported benefit with devil’s
claw in people with back pain. A doubleblind study of 117 people with back pain
reported decreased pain and improved mobility after 8 weeks’ treatment with devil’s
claw extract LI 174, known commercially as Rivoltan (Laudahn
& Walper 2001).
Use of the same extract provided significant pain relief after 4
weeks in another randomised, doubleblind placebo-controlled study of 63
subjects with muscle stiffness (Gobel et al 2001).
Similar results were reported in two double-blind studies of 118 people (Chrubasik
et al 1996) and 197 people (Chrubasik et
al 1999) with chronic lower back pain.
Devil’s claw appears to compare favourably to conventional treatments.
A 6-week double-blind study of 88 subjects comparing devil’s claw to rofecoxib found
equal improvements in both groups (Chrubasik et al 2003b) A
follow-up of the subjects from that study who were all given devil’s claw for 1
year found that it was well tolerated and improvements were sustained (Chrubasik
et al 2005). In an open, prospective study, an unspecific lower back pain
treatment with Harpagophytum extract and conventional therapy were found
to be equally effective (Schmidt et al 2005).
Three recent reviews looking at the treatment of low back pain
concluded that there is strong evidence for short-term improvements in pain and
rescue medication for devil’s claw products standardised to 50 and 100 mg
harpagoside as daily doses (Chrubasik JE et al 2007, Gagnier
et al 2006, 2007). Devil’s claw root is approved for relief of low back pain
by ESCOP (ESCOP 2003).
Dyspepsia
Traditionally, devil’s claw has also been used to treat dyspepsia
and to stimulate appetite (Fisher & Painter
1996). The bitter principles in the herb provide a theoretical basis
for its use in these conditions, although controlled studies are not available to
determine effectiveness. The herb is Commission E (Blumenthal
et al 2000) and ESCOP (2003) approved for dyspepsia and loss of appetite.
OTHER USES
Traditionally, the herb is also used internally to treat febrile
illnesses, allergic reactions and to induce sedation, and topically for wounds,
ulcers, boils and pain relief (Fisher & Painter 1996, Mills &
Bone 2000), as well as for diabetes, hypertension, indigestion and anorexia
(Van Wyk 2000).

Figure 1. Devil’s
claw (Harpagophytum procumbens).

Figure 2. Devil’s claw – dried drug substance (root).
ACTIONS
Antiinflammatory
Action
Several studies have evaluated
the antiinfl ammatory properties of devil’s claw in the treatment of joint
conditions. The results are mixed. One Canadian study (Whitehouse et al, 1983)
evaluated Harpagophytum
procumbens for reduction of rat hindfoot edema.
Devil’s claw was completely ineffective, even at doses greater than 100 times the
recommended human dose. Another study produced similar results. No clinical signifi
cance was found when human subjects consumed devil’s claw (Moussard et al, 1992).
Another study (Baghdikian et al, 1997) reported confl icting results on
harpagoside, one of the chemical components of the herb, which showed analgesic
and antiinfl ammatory properties. H. procumbens was found to produce analgesic and antiinfl ammatory
effects (Chantre et al, 2000; Fiebich et al, 2001; Gobel et al, 2000).
Another study determined that
the iridoid glycosides are responsible for the analgesic, antiinfl ammatory,
and antiphlogistic effects of devil’s claw (Wegener, 1999). Devil’s claw
possesses analgesic, antiinfl ammatory, and hypoglycemic properties as
suggested in folklore (Mahomed, 2004).
Cardiovascular
Action
When rats and rabbits were
studied to determine the cardiovascular effects of H. procumbens, a signifi cant dose-dependent reduction occurred in
arterial blood pressure, along
with a reduction in heart rate at high doses. Harpagoside, one of the chemical components of the herb, exhibited less activity than
did the extract of H.
procumbens.
The extract of H. procumbens produced a mild decrease in heart rate, with mild
positive inotropic effects at low doses but a signifi cant negative inotropic
effect at higher doses. Harpagoside showed negative chronotropic and positive
inotropic effects (Circosta et al, 1984). Another study demonstrated that
devil’s claw exerts a protective action in hyperkinetic ventricular arrhythmias
in rats (Costa De Pasquale et al, 1985).
Other Actions
Devil’s claw depresses the central nervous system and may
be used as an anticoagulant as described in folklore (Mahomed, 2006).
PHARMACOLOGICAL ACTIONS
The active constituents of devil's claw are widely held to be
the iridoid glucosides although, of these, it has not been definitively established
whether harpagoside is the most important pharmacologically active constituent
of the whole extract. Other compounds present in the root may contribute to the
pharmacological activities of devil's claw.(15, 16) It has also been suggested that
harpagogenin, formed by in vivo acid hydrolysis of harpagoside, may have
biological activity.(17)
IN VITRO AND ANIMAL STUDIES
Pharmacokinetics Transformation of the iridoids harpagide, harpagoside
and 8-O-(p-coumaroyl)-harpagide into the pyridine monoterpene alkaloid aucubinine
B, chemically or by human intestinal bacteria in vitro, has been documented.(18,
19) However, it is not known if aucubinine B is formed in vivo by intestinal bacteria
and, therefore, whether it contributes to the pharmacological activity of
devil's claw.(19)
Anti-inflammatory and analgesic
activities Animal studies of the
anti-inflammatory and analgesic activities of devil's claw have reported conflicting results. Activity appears to differ
depending on the route of administration of devil's claw, and the model of inflammation,
whether acute or subacute. Also, studies have assessed the effects of different
preparations of H. procumbens (e.g.
aqueous extracts and ethanolic extracts) and it is important to consider this
when interpreting the results.
In controlled experiments in rats, a 60% ethanol extract of H. procumbens roots injected
(compartment and site not specified) at doses of 25, 50 and 100 mg/kg body
weight daily for four days beginning five days after sub-plantar injection of
Freund's adjuvant produced a significantly greater antinociceptive response in
the hot-plate test and significantly reduced paw oedema than did control
(distilled water) on days 6–8 after induction of experimental arthritis (p <
0.01 for all).(20) Similar results were obtained when administration of H. procumbens extract was initiated 20
days after sub-plantar injection of Freund's adjuvant and continued for 20
days, with tests for antinociceptive and antiinflammatory activity performed on
four occasions during this period. Pretreatment with a dried aqueous extract of
devil's claw root at doses of 100 mg/kg and above, administered
intraperitoneally, resulted in peripheral analgesic activity demonstrated by a significant
reduction in the number of writhings induced by acetic acid in mice.(16)
However, no effect was observed in the hotplate test, indicating a lack of central
analgesic activity with devil's claw extract.
The peripheral analgesic properties of intraperitoneal dried aqueous
extract of devil's claw have been confirmed in other studies for doses of 400
mg/kg and above.(9) A subsequent series of experiments found that administration
of an aqueous extract of H. procumbens root
at doses of 200–800 mg/kg body weight intraperitoneally resulted in significantly
greater antinociceptive effects than did control in both the hot-plate and
acetic-acid induced writhings tests in mice (p < 0.05 versus control) and,
at a dose of 400 or 800 mg/kg body weight, in a significant reduction in
egg-albumin induced hind-paw inflammation in rats, compared with control (p
< 0.05).(21)
In contrast, other studies have reported that dried aqueous extract
of devil's claw administered orally had no effect on carrageenan- or
Mycobacterium butyricum- (Freund's adjuvant) induced oedema in rat paw, whereas
both indometacin and aspirin displayed significant anti-inflammatory
activity.(22, 23) However, dried aqueous extract of devil's claw administered
by intraperitoneal injection demonstrated significant activity in the
carrageenan- induced oedema test in rats, an acute model of inflammation.(16)
The effect on oedema was dose-dependent for doses of devil's claw extract
100–400 mg/kg, and reached a maximum three hours after carrageenan injection.
Other studies in rats have reported significant reductions in oedema using the same
model following pretreatment with intraperitoneal(9, 24) and intraduodenal, but
not oral, dried aqueous extract of devil's claw.(24)
Anti-inflammatory activity of harpagoside has been demonstrated in
experimental models, including the croton oil-induced granuloma pouch test, and
for harpagogenin, the aglucone of harpagoside, in the croton oil-induced
granuloma pouch test and in formalin-induced arthritis in rats.(25) Studies
have also reported peripheral analgesic and antiinflammatory properties for the
related species Harpogophytum zeyheri.(9) Animal studies using aqueous extracts
of devil's claw have suggested that the extract may be inactivated by passage through
the acid environment of the stomach.(16, 24) One study compared the
anti-inflammatory activities of aqueous devil's claw extract administered by
different routes. Intraperitoneal and intraduodenal administration led to a
significant reduction in the carrageenan-induced rat paw oedema test, but there
was no effect following oral administration.(24) In another study, aqueous devil's
claw extract pretreated with hydrochloric acid to mimic acid conditions in the
stomach showed no activity in pharmacological models of pain and
inflammation.(16)
A clear mechanism of action for the purported anti-inflammatory effects
of devil's claw has yet to be established. In vitro, devil's claw (100 mg/mL )
had no significant effect on prostaglandin (PG) synthetase activity, whereas
indometacin (316 mg/mL ) and aspirin (437 mg/mL ) caused 50% inhibition of this
enzyme.(23) In other in vitro studies in human whole blood samples, devil's
claw extracts and fractions of extracts were tested for their effects on thromboxane
B2 (TXB2) and leukotriene (LT) biosynthesis.(26) TXB2 is an end-product of arachidonic
acid metabolism by the cyclooxygenase 1 (COX-1) pathway. Inhibition appeared to
be dependent on the harpagoside content of the extracts or fractions.(26) An
aqueous extract of H. procumbens inhibited
lipopolysaccharide-induced enhancement of cyclooxygenase-2 activity, resulting
in suppression of PGE2 synthesis in in-vitro experiments using the mouse fibroblast
cell line L929.(27) In the same system, the extract inhibited inducible nitric
oxide synthase (iNOS) mRNA expression, resulting in suppression of nitric oxide
production. Inhibition of iNOS expression by an aqueous extract of H. procumbens roots, resulting in
suppression of nitrite production, has also been described following
experiments in rat renal mesangial cells. The effect was observed with a
harpagoside free extract and with an extract containing a high concentration (27%)
of harpagoside, but not with extracts containing around 2% harpagoside,
indicating that high concentrations of harpagoside as well as other
concentrations are necessary to bring about the effect.(28)
Harpagoside (100 mmol/L), but not harpagide (100 mmol/L), inhibited
calcium ionophore A23187-stimulated release of TXB2 from human platelets.(29)
However, harpagoside and harpagide had no significant inhibitory effect on
calcium ionophore A23187-stimulated release of PGE2 and LTC4 from mouse
peritoneal macrophages.(29)
Other preclinical studies have described effects for devil's claw
extracts and/or isolated constituents on other pathways involved in
inflammatory processes. In vitro inhibition of tumour-necrosisfactor- a (TNF-a)
synthesis in lipopolysaccharide-stimulated human monocytes by a hydroalcoholic
extract of devil's claw (SteiHap 69) has also been documented.(30) Inhibitory
activity against human leukocyte elastase (a serine proteinase involved in inflammatory
processes) has been reported for an aqueous extract of H. procumbens roots (drug to extract ratio 1.5-2.5 : 1) and the isolated
constituents 60-O-acetylacteoside, isoacteoside, 8-p-coumaroylharpagide, pagoside
and caffeic acid, with IC50 values of 542, 47, 179, 179, 154 and 86 mg/mL ,
respectively. The IC50 values for several other constituents, including
acteoside and harpagoside were higher than 300 mg/mL (4). An ethanol extract of H. procumbens
significantly reduced IL-1b-induced production of several matrix metalloproteinase
enzymes (MMPs) in human chondrocytes.(31) (In inflammatory diseases, there is
increased production of cytokines such as IL-1b and TNF-a, which results in an
increased production of MMPs which breakdown the extracellular cartilage
matrix.)
Other activities
Crude methanolic extracts of devil's claw have been shown to be cardioactive in
vitro and in vivo in animals. A protective action against ventricular
arrhythmias induced by aconitine, calcium chloride and epinephrine
(adrenaline)/chloroform has been reported for devil's claw given
intraperitoneally or added to the reperfusion medium.(32, 33) The crude extract
was found to exhibit greater activity than pure harpagoside.(33) In isolated
rabbit heart, low concentrations of a crude methanolic extract had mild
negative chronotropic and positive inotropic effects,(32) whereas high
concentrations caused a marked negative inotropic effect with reduction in
coronary blood flow.(32) In anaesthetised dogs, harpagoside administered orally
by gavage caused a decrease in mean aortic pressure and arterial and pulmonary
capillary pressure.(34)
In vitro, harpagoside has been shown to decrease the contractile
response of smooth muscle to acetylcholine and barium chloride on guinea-pig
ileum and rabbit jejunum. Harpagide was found to increase this response at
lower concentrations, but antagonised it at higher concentrations.(35) On the
basis of these studies in isolated smooth muscle, it was suggested that the
constituents of devil's claw may influence mechanisms regulating calcium influx.(35)
Methanolic extracts have also exhibited hypotensive properties in
normotensive rats, causing a decrease in arterial blood pressure following oral
doses of 300 mg/kg and 400 mg/kg body weight.(32) Aqueous fractions derived
from an extract of devil's claw root (drug to extract ratio 2 : 1 containing
2.6% harpagoside) showed antioxidant activity in an in-vitro assay based on
ability to scavenge 2,20-azino-bis(3-ethylbenzthiazoline-6-sulfonic acid)-derived
radicals.(36) However, harpagoside showed only weak antioxidant activity. In
mice, a methanol extract of H. Procumbens root tubers applied topically to
shaven skin 30 minutes before application of 12-O-tetradecanoylphorbol-13-acetate
(TPA), a stimulator of COX-2 expression, led to a significant reduction in
COX-2 protein when assessed four hours after TPA administration.(37) The
extract did not have any effect on TPA-induced activation of nuclear factor-kB,
but inhibited TPA-induced activation of activator protein-1, which is involved
in the regulation of COX-2 in mouse skin. Overexpression of COX-2 is thought to
be involved in tumour promotion. Antidiabetic activity has been described for
an aqueous extract of H. procumbens root
in in vivo experiments in rats with streptozotocin-induced diabetes mellitus.(21)
The extract significantly reduced blood glucose concentrations in both fasted normoglycaemic
rats and fasted diabetic rats when administered intraperitoneally at doses of
800 mg/kg body weight. T
wo diterpene constituents ((þ)-8,11,13-totaratriene-12,13-diol and
(þ)-8,11,13-abietatrien-12-ol) isolated using bioassay-guided fractionation
from a petroleum ether extract of H.
procumbens root were found to be active against a chloroquine-sensitive
(D10) and a chloroquine-resistant (K1) strain of Plasmodium falciparum in vitro (IC50 < 1 mg/mL ).(2)Devil's claw
extracts possess weak antifungal activity against Penicillium digitatum and Botrytis
cinerea.(38)
CLINICAL STUDIES
Pharmacokinetics
There is little published information on the pharmacokinetics of devil's claw
extracts in humans. A pharmacokinetic study involving a small number of healthy
male volunteers (n = 3) measured plasma harpagoside concentrations after oral
administration of devil's claw extract (WS1531 containing 9% harpagoside) 600, 1200
and 1800 mg as film-coated tablets.(26) Maximal plasma concentrations of
harpagoside were reached after 1.3–1.8 hours, and were 8.2 ng/mL and 27.8 ng/mL for doses of harpagoside of 108 and 162 mg,
respectively (corresponding to 1200 and 1800 mg devil's claw extract, respectively).
Other studies involving small numbers of healthy male volunteers indicated that
the half-life ranged between 3.7 and 6.4 hours. Other results suggested that
there may be low oral absorption or a considerable first-pass effect with
devil's claw extract, although this needs further investigation.(26)
Pharmacodynamics A
study involving healthy volunteers investigated the effects on eicosanoid
production of orally administered devil's claw (four 500-mg capsules of powder,
containing 3% glucoiridoids, daily for 21 days).(39) No statistically significant
differences on PGE2, TXB2, 6-keto-PGF1a and LTB4 were observed following the
period of devil's claw administration, compared with baseline values. By
contrast, in a subsequent study involving whole blood samples taken from
healthy male volunteers, a biphasic decrease in basal cysteinyl-leukotriene
(Cys-LT) biosynthesis, compared with baseline values, was observed following
oral administration of devil's claw extract (WS1531 containing 9% harpagoside)
600, 1200 and 1800 mg as film-coated tablets.(26)
Therapeutic activity
The efficacy and effectiveness of devil's claw have been investigated in around
20 clinical studies involving patients with rheumatic and arthritic conditions,
and low back pain.(15, 40) These studies have involved different methodological
designs, including several uncontrolled studies, and different preparations of
devil's claw, including crude drug and aqueous extracts. Evaluating the evidence
is further complicated as preparations tested in clinical trials typically have
been standar-dised for their harpagoside content and, although harpagoside is believed
to contribute to activity, it is not yet clear to what extent and which other
constituents are important. Therefore, at present, there is insufficient
evidence to draw definitive conclusions regarding the efficacy of specific
devil's claw preparations, and because of the differences in the pharmaceutical
quality of individual preparations, general conclusions on efficacy cannot be drawn.(41)
A systematic review of the quality of clinical trials involving devil's
claw found that although the results of some studies have provided evidence for
the effectiveness of certain devil's claw preparations, the quality of evidence
was not sufficient to support the use of any of the available products.(42)
A systematic review of 12 controlled, randomised or
quasirandomised trials of H. procumbens preparations
in patients with osteoarthritis (5 trials), low back pain (4 trials) and mixed
pain conditions (3 trials) found differing levels of evidence for the different
H. procumbens preparations assessed.
There was evidence (from two trials involving a total of 325 participants) that
an aqueous extract of H. procumbens administered
orally at a dose equivalent to harpagoside 50 mg daily for four weeks was superior
to placebo in reducing pain in patients with acute episodes of chronic
non-specific low-back pain.(13) There was also evidence (from one trial for
each) that the same extract administered orally at a dose equivalent to
harpagoside 100 mg daily for four weeks was superior to placebo, and at a dose
equivalent to harpagoside 60 mg daily for six weeks was not inferior
to rofecoxib 12.5 mg daily, in reducing pain in patients with acute episodes of
chronic non-specific low-back pain. There was evidence that powdered H. procumbens plant material at a dose
equivalent to 57 mg harpagoside daily for 16 weeks was not inferior to
diacerhein. Overall, however, the limited amount of data and heterogeneous
nature of the available studies, indicate that further randomised controlled
trials assessing well-characterised H.
procumbens preparations and involving sufficient numbers of patients are
required. Several of the trials mentioned above are discussed in more detail
below. A randomised, double-blind, placebo-controlled study involving 118
patients with acute exacerbations of chronic low back pain investigated the
effects of devil's claw extract 800 mg three times daily (equivalent to 50 mg
harpagoside daily) for four weeks.(43) There was no statistically significant
difference between the devil's claw and placebo groups in the primary outcome
measure –consumption of the opioid analgesic tramadol over weeks 2–4 of the
study – among the 109 patients who completed the study. This was an unusual
choice of primary outcome measure as it gives no direct indication of the
degree of pain experienced by participants. There was a trend towards improvement
in a modified version of the Arhus Low Back Pain Index (a measure of pain,
disability and physical impairment) for devil's claw recipients compared with placebo
recipients, although this did not reach statistical significance. A greater
proportion of patients in the devil's claw group were pain-free at the end of
the study, although this was only a secondary outcome measure.
On the basis of these findings, a subsequent randomised, double-blind,
placebo-controlled trial involving 197 patients with exacerbations of low back
pain tested the effects of two doses of devil's claw (WS1531) extract against
placebo.(44) Participants received devil's claw extract 600 mg or 1200 mg daily
(equivalent to 50 mg and 100 mg harpagoside daily, respectively), or placebo,
for four weeks. There was a statistically significant difference (p =0.027)
between devil's claw and placebo with respect to the primary outcome measure – the
number of patients who were pain-free without tramadol for at least five days
during the last week of the study. However, numbers of patients who were
painfree were low (3, 6 and 10 for placebo, devil's claw 600 mg daily and
devil's claw 1200 mg daily, respectively). Furthermore, this is a non-standard
outcome measure. Arhus Low Back Pain Index scores improved significantly in all
three groups, compared with baseline values, although there was no
statistically significant difference between groups.
In a randomised, double-blind, placebo-controlled study involving
patients with non-specific low back pain, 65 participants received devil's claw
extract (LI-174, Rivoltan), or placebo, 480 mg twice daily (equivalent to 24 mg
harpagoside daily) for four weeks.(45) There was a significant improvement (p
< 0.001) in visual analogue scale (VAS) scores for muscle pain in the
devil's claw group, but not the placebo group, compared with baseline values,
after two and four weeks' treatment. Differences in VAS scores between the two
groups were statistically significant after four weeks' treatment (p <
0.001). Significant differences between the two groups in favour of devil's claw
after four weeks' treatment were also observed with several other parameters,
including muscle stiffness and muscular ischaemic pain.
A small number of studies has compared the efficacy of devil's claw
with that of conventional pharmaceutical agents in the treatment of low back
pain. In a randomised, double-blind, pilot trial, 88 participants with acute
exacerbations of low back pain received an aqueous extract of devil's claw
(Doloteffin; drug to extract ratio 1.5-2.5:1) 2400 mg daily in three divided
doses (equivalent to 60 mg harpagoside daily), or rofecoxib (Vioxx) 12.5 mg
daily for six weeks.(46) At the end of this period, compared with baseline
values, there were improvements in Arhus Low Back Pain Index scores, health
assessment questionnaire scores, and increases in the numbers of pain-free
patients for both groups. There were no statistically significant differences
between groups for any of the outcome measures but, because the study did not
include sufficient numbers of patients, these findings do not demonstrate
clinical equivalence between the two treatments.(46)
A randomised, double-blind, pilot trial in which 88 participants
with acute exacerbations of low back pain received an aqueous extract of
devil's claw (Doloteffin), or rofecoxib (Vioxx) for six weeks offered
participants continuing treatment with devil's claw aqueous extract two tablets
three times daily for up to one year after the six-week pilot study. Participants
were not aware of their initial study group (i.e. devil's claw extract or
rofecoxib) until towards the end of the one-year follow-up study.(47) In total,
38 and 35 participants who had previously received devil's claw and rofecoxib,
respectively, participated in the follow-up study, and underwent assessment
every six weeks. After 24 and 54 weeks, 53 and 43 participants, respectively,
remained in the study. There were no convincing differences between the two
groups (i.e. those who previously received devil's claw and those who received
rofecoxib) with respect to pain scores, use of additional analgesic medication,
Arhus Index scores and health assessment questionnaire scores.
Furthermore, the uncontrolled design of the follow-up study would
have precluded any definitive conclusions regarding differences between the two
groups. A randomised, double-blind trial compared the efficacy of devil's claw
extract with that of diacerein in 122 patients with osteoarthritis of the knee
and hip.(14) Participants received powdered cryoground devil's claw (Harpadol)
2.61 g daily, or diacerein 100 mg daily, for four months.
VAS scores for spontaneous pains improved significantly in both
groups, compared with baseline values, and there were no differences
between devil's claw and diacerein with respect to VAS scores.
In a placebo-controlled study involving 89 patients with rheumatic
complaints, devil's claw recipients (who received powdered
crude drug 2 g daily for two months) showed significant improvements
in sensitivity to pain and in motility (as measured by
the finger-to-floor distance), compared with placebo recipients.(48)
Several, open, uncontrolled, post-marketing surveillance studies(
49–53) have assessed the effects of devil's claw preparations in patients with
rheumatic and arthritic disorders, and back pain. These studies typically have
reported improvements in pain scores at the end of the treatment period,
compared with baseline values. However, the design of these studies (i.e. no
control group) does not allow any conclusions to be drawn on the effects of
devil's claw in these conditions as there are alternative explanations for the
observed effects.
Another study involved 45 patients with osteo- or rheumatoid arthritis
who received devil's claw root extract 2.46 g daily for two weeks in addition
to non-steroidal anti-inflammatory drug (NSAID) treatment, followed by devil's
claw extract alone, for four weeks.(54) It was reported that there were no
statistically significant changes in pain intensity and duration of morning stiffness
during the period of treatment with devil's claw extract alone. In subgroups of
patients with rheumatoid arthritis and those with osteoarthritis, small decreases
were observed in concentrations of C-reactive protein and creatinine,
respectively.
The design of this study in terms of the treatment regimen (NSAID
followed by devil's claw extract without a wash-out period), also precludes
definitive conclusions about the effects of devil's claw preparations.
MAIN ACTIONS
Anti-inflammatory/Analgesic
There is good in vitro and in vivo pharmacological evidence of the
anti-inflammatory and analgesic properties of devil’s claw, although some
negative findings have also been reported (McGregor et al 2005).
Overall, greatest activity appears to be in semi-chronic rather than acute
conditions. Devil’s claw exerted significant analgesic effects against
thermally and chemically induced nociceptive pain stimuli in mice and
significant dose-related reduction of experimentally induced acute inflammation
in rats (Mahomed & Ojewole 2004), as well as reducing pain
and inflammation in Freund’s adjuvant- induced arthritis in rats (Andersen
et al 2004). Results from a recent study in mice suggest that the opioid
system is involved in the antinociceptive effects of H. procumbens extract
(Uchida et al 2008).
The iridoids, particularly harpagoside, are thought to be the main
active constituents responsible for the anti-inflammatory activity, although
the mechanism of action is unknown and devil’s claw is also rich in
water-soluble antioxidants (Betancor- Fernandez
et al 2003). More recent in vitro evidence suggests that the
anti-inflammatory effect may in part be due to antioxidant activity (Denner 2007,
Grant et al 2009, Langmead et al 2002).
A study administering H. procumbens extract
intraperitoneally to rats found that the anti-inflammatory response does not
depend on the release of adrenal corticosteroids (Catelan
et al 2006). Contradictory evidence exists as to whether devil’s claw
affects prostaglandin (PG) synthesis. Early in vitro and in vivo studies
suggest that it does not inhibit PG synthesis (Whitehouse et al
1983) and this is supported by studies of PG production in humans (Moussard
et al 1992). However, more recent investigations have suggested that its
anti-inflammatory and analgesic activities are due to suppression of PGE2
synthesis and nitric oxide production and that the herb may suppress
expressions of COX-2 and iNOS (Jang et al 2003).
Harpagoside alone has been shown to suppress COX-2 and iNOS at both the mRNA
and protein level in vitro due to a suppression of NF-kappaB activation (Huang
et al 2006).
Recent in vitro research shows that harpagoside and 8-O-(p-coumaroyl)-harpagide
exhibit a greater reduction in COX-2 expression than verbascoside and that
harpagide on the other hand causes a significant increase in COX-2 expression
(Abdelouahab & Heard 2008a). Additionally, methanolic extracts of devil’s
claw have been shown to inhibit COX-2 in vivo (Kundu et al 2005,
Na et al 2004). Inhibition of leukotriene synthesis has been observed in vitro,
which appears to relate to the amount of harpagoside present (Loew
et al 2001).
A study using subcritical and supercritical CO2 extracts (15 to
30% harpagoside) showed almost total inhibition of 5-lipoxygenase biosynthesis
at 51.8 mg/mL of extract, whereas the
conventional extract (2.3% harpagoside) did not inhibit the enzyme
significantly (Gunther et al 2006).
In vivo experiments have determined that the method of administration
of devil’s claw affects its anti-inflammatory properties. Intraperitoneal and intraduodenal
administration was shown to reduce carrageenan-induced oedema, whereas oral
administration had no effect, suggesting that exposure to stomach acid may
reduce its anti-inflammatory activity (Soulimani et al 1994).
This is supported by a study that found a loss of anti-inflammatory activity
after acid treatment (Bone & Walker 1997). devil’s claw may be used
as an anti-inflammatory agent in the treatment of glomerular inflammatory diseases
(Kaszkin et al 2004a). Devil’s claw extract produced
a concentration-dependent suppression of nitrite formation in rat mesangial
cells in vitro due to an inhibition of iNOS expression through interference
with the transcriptional activation of iNOS. It was found that this activity
was due to harpagoside, together with other constituents that possibly have
strong anti-oxidant activity (Kaszkin et al 2004b). It
has been suggested that the suppression of inflammatory cytokine synthesis,
demonstrated in vitro and vivo (Fiebich et al 2001,
Spelman et al 2006), could explain its therapeutic effect in arthritic inflammation
(Kundu et al 2005). Fiebich and co-workers found that a
60% ethanolic extract decreases the expression of IL-1-beta, IL-6, and TNF-alpha
(Fiebich et al 2001).
Chondroprotective
In
vitro data suggest that the active principles of H. procumbens inhibit not
only inflammatory mediators but also mediators of cartilage destruction, such
as matrix metalloproteinases, NO and elastase (Boje et al 2003,
Schulze-Tanzil et al 2004). A study using an animal model confirmed a chondroprotective
effect in which the tissue inhibitor of metalloproteinase- 2 is involved (Chrubasik
et al 2006).
Hypoglycaemic
Devil’s
claw extract produced a dose-dependent, significant reduction in the blood
glucose concentrations of both fasted normal and fasted diabetic rats (Mahomed
& Ojewole 2004).
OTHER ACTIONS
In
vitro and in vivo evidence suggests that harpagoside may exhibit cardiac affects
and lower blood pressure, heart rate and reduce arrhythmias (Fetrow
& Avila 1999). As an extremely bitter herb, devil’s claw is thought to increase
appetite and bile production. Diterpenes extracted from the roots and seeds of
devil’s claw exhibited selective antiplasmodial (Clarkson et al 2003)
and antibacterial activity (Weckesser et
al 2007) in vitro, which may have future relevance in view of the increasing
resistance to conventional antimalarials and antibiotics. One study showed that
aqueous devil’s claw extract can markedly delay the onset, as well as reduce
the average duration, of convulsion in mice. Although not conclusive, it seems that
the extract produces its anticonvulsant activity by enhancing GABAergic neurotransmission
and/or facilitating GABAergic action in the brain (Mahomed &
Ojewole 2006).
ACTIVITIES
Allergenic (f; PHR); Analgesic (2; CAN; KOM; MAB;
PH2); Antiarrhythmic (1; APA); Antiarthritic (1; CRC; MAB; PH2; VVG); Antiedemic
(1; BGB); Antiexudative (f; SHT); Antiinflammatory (2; APA; BGB; CRC; KOM;
PH2); Antipyretic (f; HHB); Antirheumatic (1; CAN; MAB); Aperitif (2; APA; HH2;
KOM; VAG); Bitter (1; APA; MAB; PED); Choleretic (2; HH2; KOM; PH2); Depurative
(f; BGB; PED); Digestive (f; SKY); Diuretic (f; CAN); Hypocholesterolemic (1;
CRC; PED; VAG); Hypotensive (1; APA; BGB); Hypouricemic (1; CRC; PED; VAG);
Laxative (f; MAB; WBB); Secretagogue (1; PH2); Sedative (f; CAN); Tonic (1;
APA; MAB; VVG); Uricolytic (1; APA); Uterocontractant (f; VAG).
INDICATIONS
Aging (f; CRC); Allergy (1; BGB; CRC; MAB; PH2);
Anorexia (2; APA; HH2; KOM; PH2; SHT; VAG); Arrhythmia (1; APA; BGB; MAB);
Arthrosis (2; APA; CRC; KOM; MAB; PH2; VVG); Atherosclerosis (f; CRC); Backache
(2; BGB; BRU; MAB; PHR); Blood (f; BGB); Boil (1; BGB; CRC; MAB; VVG); Bursitis
(f; WAF); Cancer (f; APA; WBB); Cancer, skin (f; CRC); Cardiopathy (1; MAB);
Childbirth (1; APA; BRU; CRC; MAB; VAG; WBB); Cholecystosis (2; CRC; PHR; PH2);
CNS (f; PH2); Cramp (f; VAG); Cystosis (f; CRC; HHB; PH2); Dermatosis (f; BGB;
PHR); Diabetes (f; CRC; HHB; VAG); Dysmenorrhea (1; CRC; VAG); Dyspepsia (2;
APA; BGB; CRC; KOM; PH2; SHT); Edema (1; BGB); Enterosis (f; BRU; CRC); Fever
(1; APA; BGB; BRU; HHB; VAG); Fibromyalgia (f; WAF); Fibrosis (1; CAN; VAG); Gastrosis
(f; BRU; CRC); Gout (1; CAN; CRC; VAG); Headache (1; APA; BGB; MAB); Heartburn (2;
CRC; KOM; SKY); Hepatosis (2; CRC; PHR; PH2); High Blood Pressure (1; APA; BGB;
VAG); High Cholesterol (1; CRC; PED; VAG); Inflammation (2; APA; BGB; CRC; KOM;
MAB; PH2); Insomnia (f; CAN); Lumbago (1; BGB; CAN; CRC); Migraine (1; MAB);
Myalgia (f; CAN); Nephrosis (f; CRC; HHB; PH2); Nervousness (f; CAN); Neuralgia
(1; BGB; CRC); Neurosis (f; PH2); Osteoarthrosis (1; VAG); Pain (2; APA; BGB;
CAN; KOM; MAB; PHR; PH2; VVG); Parturition (f; VVG); Pleurodynia (f; CAN);
Pregnancy (f; APA; PH2); Rheumatism (2; CAN; KOM; MAB; PHR; PH2); Sore (1; BGB;
CRC; MAB; VVG); Swelling (1; BGB); Tendinitis (1; BGB; WAF); Tuberculosis (f;
VAG); Ulcer (f; CRC; MAB); Water Retention (f; CAN); Wound (f; CRC; PHR).
I suppose that Commission E is talking about various
degenerative arthritic conditions when they approve this for, “Supportive
therapy of degenerative disorders of the locomotor system,” but just couldn’t
bring themselves around to saying arthrosis, or degenerative joints and/or
muscles (KOM).
INDICATIONS AND
USAGE
Approved by
Commission E:
• Dyspeptic complaints
• Loss of appetite
• Rheumatism
Unproven Uses: In folk medicine,
Devil's Claw is used as an ointment for skin injuries and disorders. The dried
root is used for pain relief; pregnancy discomforts; arthritis; allergies; metabolic
disorders; and kidney, bladder, liver and gallbladder disorders. In South Africa
it is used for fevers
and
digestive disorders. Devil's Claw is also used for supportive
therapy of degenerative disorders of the CNS system.
Homeopathic Uses:
Chronic
rheumatism is the primary use for Devil's Claw in homeopamy.
PRODUCT AVAILABILITY
Capsules, Dried Powdered Root, Dry
Solid Extract, Tea, Tincture
PLANT PARTS USED: ROOTS, Tubers (Secondary Root Tuber)
DOSAGES
DOSAGES
Anorexia
·
Adult PO infusion: 1.5 g herb
tid (Blumenthal, 1998)
Gout
·
Adult PO dried powdered root:
1-2 g tid (Murray, Pizzorno, 1998)
·
Adult PO tincture: 4-5 mL (1:5 dilution) tid (Murray, Pizzorno, 1998)
·
Adult PO dry solid extract: 400
mg tid (Murray, Pizzorno, 1998)
Osteoarthritis
·
Adult PO dried powdered root:
1-2 g tid (Murray, Pizzorno, 1998)
·
Adult PO tincture: 4-5 mL (1:5 dilution) tid (Murray, Pizzorno, 1998)
·
Adult PO dry solid extract: 400
mg tid (Murray, Pizzorno, 1998)
Other
·
Adult PO infusion: _4.5 g herb (Blumenthal, 1998) in 300 mL boiling water, let stand 8 hr, strain and
drink
DOSAGES
Dosages
for oral administration (adults) recommended in older and more contemporary
standard herbal reference texts are given below.
Painful Arthrosis and Tendonitis
·
1.5–3 g dried tuber as a decoction, three times daily; 1–3 g
drug or equivalent aqueous or hydroalcoholic extracts;(G76)
·
Liquid Extract 1–3mL (1 :
1, 25% ethanol) three times daily.(G6)
Loss Of Appetite Or Dyspepsia
·
Dried Tuber 0.5 g as a decoction, three times
daily.(G6)
·
Tincture 1
mL (1 : 5, 25% ethanol) three times
daily.(G6)
Clinical
trials of devil's claw root extracts for the treatment of low back pain
typically have tested oral doses ranging from 2000– 4500 mg daily, in two or
three divided doses (equivalent to less than 30 mg up to 100 mg harpagoside
daily, depending on the particular extract), for four to 20 weeks.(13) In a
clinical trial in osteoarthritis, participants received capsules containing
powdered cryoground devil's claw root 2610 mg daily for four months.(14)
DOSAGES
·
1 tsp chopped root/2 cups water, sipped through day (APA); 1.5–4.5(–10)
g root (KOM; SHT; SKY);
·
6 g root/day (MAB); 1–2 tsp fresh root (PED); 0.5–1 g dry root
(PED);
·
1 g dry root:5 mL alcohol/5 mL water (PED); 0.1–0.25 g powdered tuber (PNC);
·
0.1–0.25 g dry tuber as tea 3 x/day (CAN); 0.1–0.25 mL liquid extract (1:1 in 25% ethanol) 3 x /day (CAN);
·
6–12 mL liquid extract
(1:2)/day (MAB); 15–30 mL tincture
(1:5)/day (MAB);
·
0.5–1 mL root tincture
(1:5 in 25% alcohol) 3 x /day (CAN).
DOSAGES
Musculoskeletal Conditions
·
Dried root or equivalent
aqueous or hydroalcoholic extracts: 2–6 g daily for painful arthritis; 4.5–9 g
daily for lower back pain.
·
Liquid extract (1:2):
6–12 mL /day.
·
Tincture (1:5): 2–4 mL
three times daily.
It is suggested that devil’s claw extracts with at least 50 mg
harpagoside in the daily dosage should be recommended for the treatment of pain
(Chrubasik 2004a, 2004b).
Digestive Conditions (e.g. dyspepsia)
·
Dosages equivalent to
1.5 g/day dried herb are used (Blumenthal et al
2000). It is suggested that devil’s claw
preparations be administered between meals, when gastric activity is reduced.
DOSAGES
MODE
OF ADMINISTRATION: As comminuted drug for infusions and
other preparations for internal use, as an ointment for external use.
HOW SUPPLIED:
•
Capsules
— 405 mg, 480 mg, 510 mg, 520 mg
•
Tablets
PREPARATION: To make an
infusion, use 1 teaspoonful (equivalent to 4.5 g) comminuted drug with 300 mL boiling water. Steep for 8 hours and strain.
DAILY
DOSAGE:
for
loss of appetite, the recommended dosage is 1.5 g of drug; otherwise 4.5 g of
drug is used. The infusion can be taken 3 times a day.
HOMEOPATHIC
DOSAGE:
5
to 10 drops, 1 tablet or 5 to 10 globules 1 to 3 times a day, or from D3 1 mL injection solution sc twice weekly (HAB1). The
ointment is applied 1 to 3 times a day. For external use, 1 dessertspoon of the
tincture should be diluted with 250 mL and used for washes or poultices.
STORAGE: Store Devil's
Claw in a container that protects it from light and moisture.
PRECAUTIONS AND ADVERSE REACTIONS
Health
risks or side effects following the proper administration of designated
therapeutic dosages are not recorded. The drug has a sensitizing effect.
Devil’s claw is a well tolerated treatment. In a recent review of
28 clinical trials it was found that only minor adverse events, mainly mild
gastrointestinal symptoms (e.g. diarrhoea), occur in 3% of the patients. The incidence
of adverse effects in the treatment groups was never higher than in the placebo
groups for all 28 trials (Vlachojannis et al 2008).
Use cautiously in patients with gastric and duodenal ulcers,
gallstones or acute diarrhoea, as devil’s claw may cause gastric irritation (Blumenthal
et al 2000).
CONTRAINDICATIONS, INTERACTIONS, AND SIDE EFFECTS
CLASS 2B, 2D (AHP). Contraindicated in duodenal and gastric
ulcers (AHP, 1997). Commission E reports contraindications in GI ulcer (AEH).
Contraindicated in people with diabetes. Excessive doses may interfere with blood
pressure and cardiac therapy (CAN). LD50 = >13,500 mg/kg orl mouse (CAN).
CONTRA-INDICATIONS,
WARNINGS
Devil's claw is stated to be contra-indicated in gastric and duodenal
ulcers,(G3, G76) and in gallstones should be used only after consultation with
a physician.(G3)
Drug Interactions None have been described for devil's claw preparations.
However, on the basis of pharmacological evidence of devil's claw's
cardioactivity, the possibility of excessive doses interfering with existing
treatment for cardiac disorders or with hypo/hypertensive therapy should be
considered. Inhibitory effects on certain cytochrome P450 (CYP) drug
metabolising enzymes have been documented for a devil's claw root extract
(Bioforce) in vitro using a technique involving liquid chromatography-mass spectrometry
and automated online extraction.(58) Mean (standard deviation) IC50 values for
the devil's claw extract when tested in assays with individual CYP enzymes were
997 (23), 254 (17), 121 (8), 155 (9), 1044 (80) and 335 (14) for the CYPs 1A2,
2C8, 2C9, 2C19, 2D6 and 3A4, respectively.
Pregnancy And Lactation It
has been stated that devil's claw has oxytocic properties,(59) although the
reference gives no further details and the basis for this statement is not
known. In addition, there is no further evidence to substantiate the statement.
However, given the lack of data on the effects of devil's claw taken during
pregnancy and lactation, its use should be avoided during these periods.
CONTRAINDICATIONS
The drug should
not be used in the presence of stomach or duodenal ulcers, due to the drug's stimulation
of gastric juice secretion.
PREGNANCY USE
Devil’s claw is
not recommended in pregnancy, as it has exhibited oxytocic activity in animals.
CONTRAINDICATIONS
Pregnancy category is 3;
Breastfeeding category is 2A. Until more research is available,
this herb should not be given to children. Persons with peptic or duodenal
ulcer disease, cholecystitis, or hypersensitivity to this herb should avoid the
use of devil’s claw.
SIDE EFFECTS/ADVERSE REACTIONS
CNS: Headache
CV: Hypotension
EENT: Tinnitus
GI: Nausea,
vomiting, anorexia
INTEG: Hypersensitivity
reactions
INTERACTIONS
Drug
Antacids, H2-blockers, proton pump inhibitors: Devil’s claw may decrease the action of these agents
(Jellin et al, 2008).
Antiarrhythmics, antihypertensives: Because two of the chemical components in devil’s claw
exert inotropic and chronotropic effects, use this herb cautiously with
antiarrhythmics and antihypertensives (theoretical).
Antidiabetics: Devil’s
claw may cause an additive effect with antidiabetics (Jellin et al, 2008).
Warfarin: Devil’s
claw taken with warfarin may cause risk of bleeding (Jellin et al, 2008).
Lab Test
APTT, PT: Devil’s
claw may increase these levels.
SIGNIFICANT INTERACTIONS
Devil’s
claw has been found to moderately inhibit cytochrome P450 enzymes (CYP2C9,
2C19, 3A4) in vitro (Unger & Frank 2004), however, the clinical relevance
of this is yet to be determined. In contrast to NSAIDs, devil’s claw does not
affect platelet function (Izzo et al 2005).
Warfarin
Rare
case reports suggest that devil’s claw may potentiate the effects of warfarin,
but the reports are mostly inconclusive (Argento et al 2000, Heck
et al 2000, Izzo et al 2005). Clinical testing would be
required to confirm a possible interaction.
Anti-arrythmic
Drugs
Theoretical
interaction exists when the herb is used in high doses; however, clinical
testing is required to determine significance — observe patients taking concurrent
antiarrythmics (Fetrow & Avila 1999).
EFFECTS
Devil's Claw
stimulates gastric juice secretion and is choleretic. Anti-inflammatory, analgesic
(and tiius anti-arthritic) effect has been shown in animal experiments.
TOXICITY
The
acute LD50 of devil’s claw was more than 13.5 g/kg according to one study (Bone
& Walker 1997). In a recent review of 28 clinical trials only a few reports on
acute toxicity were found, whereas no reports on chronic toxicity had been
reported. The review concluded that more studies for longterm treatment are
needed (Vlachojannis et al 2008).
An earlier review looking at 14 clinical trials had come to the same conclusion
(Brien et al 2006).
SIDE-EFFECTS, TOXICITY
The
mechanism of action of devil's claw remains unclear, in particular, whether it
has significant effects on the mediators of acute inflammation. Data from in
vitro and clinical studies in this regard do not yet give a clear picture (see Pharmacological
Actions, In vitro and animal studies and Clinical studies, Pharmacodynamics).
It has been stated that adverse effects associated with the use of NSAIDs are
unlikely to occur with devil's claw, even during long-term treatment.(G50, G76)
While there are no documented reports of gastrointestinal bleeding or peptic
ulcer associated with the use of devil's claw, the latter statement requires
confirmation. Use of devil's claw in gastric and duodenal ulcer is
contraindicated, although this appears to be because of the drug's bitter
properties.(G50)
CLINICAL DATA
Randomised,
placebo-controlled trials involving patients with rheumatic and arthritic
conditions who have received devil's claw extracts or powdered drug at approximately
recommended doses for four weeks have reported mild, transient gastrointestinal
symptoms (such as diarrhoea, flatulence) in a small proportion (less than 10%)
of devil's claw recipients.(43–45) No serious adverse events were reported,
although one patient withdrew from one study because of tachycardia.(43)
A small number of reports of randomised trials comparing the effects
of devil's claw preparations with those of standard pharmaceutical agents has
included data on adverse events. In a randomised, double-blind, pilot trial, 88
participants with acute exacerbations of low back pain received an aqueous
extract of devil's claw (Doloteffin; drug to extract ratio 1.5-2.5:1) 2400 mg daily
in three divided doses (equivalent to 60 mg harpagoside daily), or rofecoxib
(Vioxx) 12.5 mg daily for six weeks.(46) In total, 28 (32%) participants (14 in
each group) experienced adverse events, most commonly gastrointestinal
complaints (9 in each group).
In a follow-up study, participants in the six-week pilot study were
offered continuing treatment with devil's claw aqueous extract two tablets
three times daily for up to one year. Participants were not aware of their
initial study group (i.e. devil's claw extract or rofecoxib) until towards the
end of the oneyear follow-up study.(47) In total, 38 and 35 participants who
had previously received devil's claw and rofecoxib, respectively, participated
in the follow-up study and, after 24 and 54 weeks, a total of 53 and 43
participants, respectively, remained in the study. Overall, 17 (23%) of the 73
participants in the follow-up study experienced a total of 21 adverse events.
Of these, the causality for three events was classified (by a physician not involved
in the study) as 'likely' (one allergic skin reaction) or 'possible'
(diarrhoea, acid 'hiccup') with respect to devil's claw treatment. Five
participants (7%) withdrew from the study because of adverse events. In a
randomised, controlled trial comparing devil's claw extract with diacerein in
patients with osteoarthritis, numbers of patients ending the study prematurely
because of suspected adverse drug reactions were 8 and 14 for devil's claw and
diacerein recipients, respectively.(14) In total, 26 diacerein recipients and
16 devil's claw recipients reported one or more adverse events (p = 0.042). The
numbers of adverse events attributed to the treatment was significantly lower
for devil's claw than for diacerein (10 versus 21; p = 0.017). The most frequently
reported adverse event, diarrhoea, occurred in 8.1% and 26.7% of devil's claw
and diacerein recipients, respectively.
Several, open, uncontrolled studies,(51–53) which have assessed the
effects of devil's claw preparations in patients with arthritic disorders and
back pain, have reported data on adverse events. In an open, uncontrolled,
multicentre, surveillance study involving patients with arthrosis of the hip or
knee, 75 participants received tablets containing an aqueous extract of the
secondary tubers of devil's claw (Doloteffin; drug extract ratio = 1.5-2.5 : 1)
at a dosage of two 400 mg tablets three times daily (equivalent to 50 mg
iridoidglycosides, calculated as harpagoside) for 12 weeks.(51) During the
study, four (5%) participants experienced adverse events (dyspeptic complaints,
2; sensation of fullness, 1; panic attack, 1), although none stopped treatment
with devil's claw. Causality was assessed as 'possible' for two of these events.
In a similar open, uncontrolled, multicentre study, 130 participants
with chronic non-radicular back pain received tablets containing 480 mg devil's
claw extract (LI-174; drug extract ratio = 4.4-5 : 1) at a dosage of one tablet
twice daily for eight weeks.(52)
Overall, 13 (10%) participants withdrew from the study for various
reasons, including no apparent improvement in their condition. No serious
adverse events were reported, but three partipants reported minor adverse
events (bloating, insomnia and outbreaks of sweating). In a post-marketing
surveillance study, 250 patients with non-specific low back pain or
osteoarthritic pain of the knee or hip received an aqueous extract of H. procumbens (Doloteffin) at an oral
dose equivalent to harpagoside 60 mg daily in three divided doses for eight
weeks in addition to any existing treatment and/or additional analgesic
medicines as required. Fifty participants experienced adverse events; most
commonly gastrointestinal complaints (n = 22); two participants experienced allergic
skin reactions.(53) In 27 participants, the adverse event was considered by an
independent investigator to be possibly (n = 11), likely (15) or certainly (1)
related to ingestion of devil's claw.
In another open, uncontrolled study, one patient withdrew after four
days' treatment with devil's claw aqueous extract 1.23 g daily because of
several symptoms, including frontal headache, tinnitus, anorexia and loss of
taste.(55)
There is an isolated report of conjunctivitis, rhinitis and respiratory
symptoms in a 50-year-old woman who had experienced chronic occupational
exposure to devil's claw.(56)
PRECLINICAL DATA
Acute
and subacute toxicity tests in rodents have demonstrated low toxicity of
devil's claw extracts. In a study in mice, the acute oral lethal dose (LD) LD0
and LD50 were greater than 13.5 g/kg body weight.(23) In rats, clinical,
haematological and gross pathological findings were unremarkable following
administration of devil's claw extract 7.5 g/kg by mouth for seven days.
Hepatic effects (liver weight, and concentrations of microsomal protein and
several liver enzymes) were not observed following oral treatment with devil's
claw extract 2 g/kg for seven days.(23) Other studies in mice have reported
acute oral acute intravenous LD0 values of greater than 4.64 g/kg and greater
than 1 g/kg, respectively.(57) For an extract containing harpagoside 85%, acute
oral LD0, acute intravenous LD0 and acute intravenous LD50 values were greater
than 4.64 g/kg, 395 mg/kg and 511 mg/kg, respectively.(57)
CLIENT CONSIDERATIONS
ASSESS
·
Assess for hypersensitivity
reactions. If present, discontinue use of devil’s claw and administer
antihistamine or other appropriate therapy.
·
Assess cardiac status in any
client with a cardiac condition: blood pressure, character of pulse.
·
Identify what prescription
drugs and herbal supplements the client is taking to treat this condition (see
Interactions).
·
Assess joint pain and infl
ammation in any client with an arthritic condition: pain location, duration,
intensity, and alleviating and aggravating factors.
ADMINISTER
·
Instruct the client to store
devil’s claw products in a cool, dry place, away from heat and moisture.
TEACH CLIENT/FAMILY
·
Inform the client that
pregnancy category is 3 and breastfeeding category is 2A.
·
Caution the client not to use
devil’s claw in children until more research is available.
PRACTICE POINTS/PATIENT COUNSELLING
·
Devil’s
claw reduces pain and inflammation and is a useful treatment in arthritis and
back pain, according to controlled studies.
·
The
anti-inflammatory action appears to be different to that of NSAIDs and has not
been fully elucidated. There is also preliminary evidence of a
chondroprotective effect.
·
Preliminary
research suggests that it is best to take devil’s claw between meals, on an
empty stomach.
·
Devil’s
claw appears to be relatively safe but should not be used in pregnancy and
should be used with caution in people with ulcers or gallstones
or in those taking warfarin.
PATIENTS’ FAQs
What
will this herb do for me?
Devil’s claw is a useful
treatment for arthritis and back pain. It may also increase appetite and
improve digestion and dyspepsia.
When
will it start to work?
Results from studies suggest
that pain-relieving effects will start within 4–12 weeks reaching maximum pain
relief after 3–4 months (Chrubasik S et al 2007, Thanner et al 2008).
Are
there any safety issues?
Devil’s claw should be used
cautiously by people with gallstones, diarrhoea, stomach ulcers and those taking
the drug warfarin. It is also not recommended in pregnancy.
PREPARATIONS
PROPRIETARY SINGLE-INGREDIENT
PREPARATIONS
France:
Harpadol; Harpagocid. Germany: Ajuta; Allya; Arthrosetten H; Arthrotabs;
Bomarthros; Cefatec; Dolo- Arthrodynat; Dolo-Arthrosetten H; Doloteffin;
flexi-loges; Harpagoforte Asmedic; HarpagoMega; Harpagosan; Jucurba; Matai;
Pargo; Rheuferm Phyto; Rheuma-Sern; Rivoltan; Sogoon; Teltonal; Teufelskralle.
Spain: Fitokey Harpagophytum; Harpagofito Orto.
PROPRIETARY MULTI-INGREDIENT
PREPARATIONS
Australia:
Arthriforte; Arthritic Pain Herbal Formula 1; Bioglan Arthri Plus; Boswellia
Compound; Devils Claw Plus; Extralife Arthri-Care; Guaiacum Complex; Herbal
Arthritis Formula; Lifesystem Herbal Formula
1 Arthritic Aid; Prost-1. Czech Republic: Antirevmaticky Caj. France: Arkophytum.
Germany: Dr Wiemanns Rheumatonikum. Italy: Bodyguard; Nevril; Pik Gel.
Malaysia: Celery Plus. Spain: Dolosul; Natusor Harpagosinol.


EXTRACTS
German
clinical studies confirm arthritic relief; hypocholesterolemic, hypouricemic
(PED). Chrubasik et al. (1996) studied the effectiveness in treatment of
acute low back pain. While animal studies exhibit analgesic and
antiinflammatory activities (due to harpagoside), this study of 118 patients
with nonspecific low-back pain (most for more than 15 years),with 400 mg
extract 3 ×/day (equivalent of 6000 mg crude root extract = 50 mg harpagoside).
Only 9 of the treated patients improved cf 1 in the placebo controls. The
insignificant reduction in pain was confined to those whose pain did not
radiate to one or both legs. “There was a notable absence of identifiable
clinical, hematological, or biochemical side effects” (PHM3:1). None of these
authors commented on the presence of 3 COX-2 inhibitors as well, kaempferol,
oleanolic acid, and ursolic acid.
REFERENCE
Barnes, J., Anderson, L. A., and Phillipson, J. D. 2007. Herbal
Medicines Third Edition. Pharmaceutical Press. Auckland and
London.
Braun
Duke, J. A. with Mary Jo Bogenschutz-Godwin, Judi duCellier, Peggy-Ann K.
Duke. 2002. Handbook of Medicinal Herbs 2nd Ed. CRC Press
LLC. USA.
Gruenwald, J., Brendler,
T., Jaenicke, Ch. 2000. PDR for Herbal
Medicines. Medical Economics Company, Inc. at Montvale, NJ
07645-1742. USA
Linda S-Roth. 2010. Mosby’s Handbook Of Herbs & Natural
Supplements, Fourth Edition. Mosby Elsevier. USA